A small pipeline leak (estimated 2 bbl spill) at an onshore booster station is having a major impact on Gulf of Mexico production. Per Reuters, as much as 600,000 bopd could be temporarily shut-in. GoM production averaged 1.6 million bopd in May.
These major platforms are reported to be shut-in:
Shell: Mars, Ursa, and Olympus
Chevron: Jack/St. Malo, Tahiti, and Big Foot
Equinor: Titan
Shell, the pipeline operator, did not provide an estimate on the resumption of production.
Chevron may be the only GoM operator to own its helicopter fleet. Data on their safety performance relative to GoM helicopter contractors do not appear to be available online.
Their news release focuses on hurricane preparedness and the benefits of owning their fleet. I’m not sure how significant these advantages are given that other companies can ensure similar availability through their contracts. A comparative analysis would be of interest.
“Other companies that depend on contracted helicopters to evacuate can’t create their own schedule and might have to start departing the platform days in advance,” said Jose Jaramillo, manager of Chevron’s aircraft operations in the Gulf of Mexico. “With our own helicopters on standby, we have more flexibility in determining when to safely shut down the platform, and after the storm passes, we can quickly remobilize, assess our facilities and bring production back online days faster.”
The leading causes, not all inclusive, of the accidents since 1999 are listed below, and secondary causes of these events include 13 related to helideck size or design related issues. • 21 engine related, • 25 loss of control or improper procedures, • 18 helideck obstacle strikes, • 13 controlled flight into terrain, and • 12 other technical failures
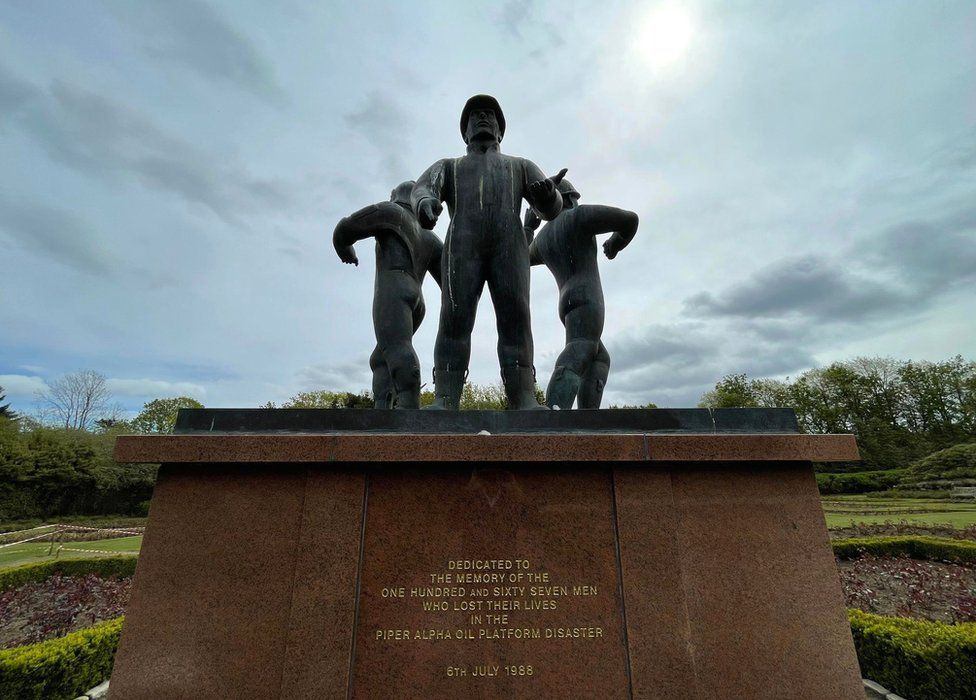
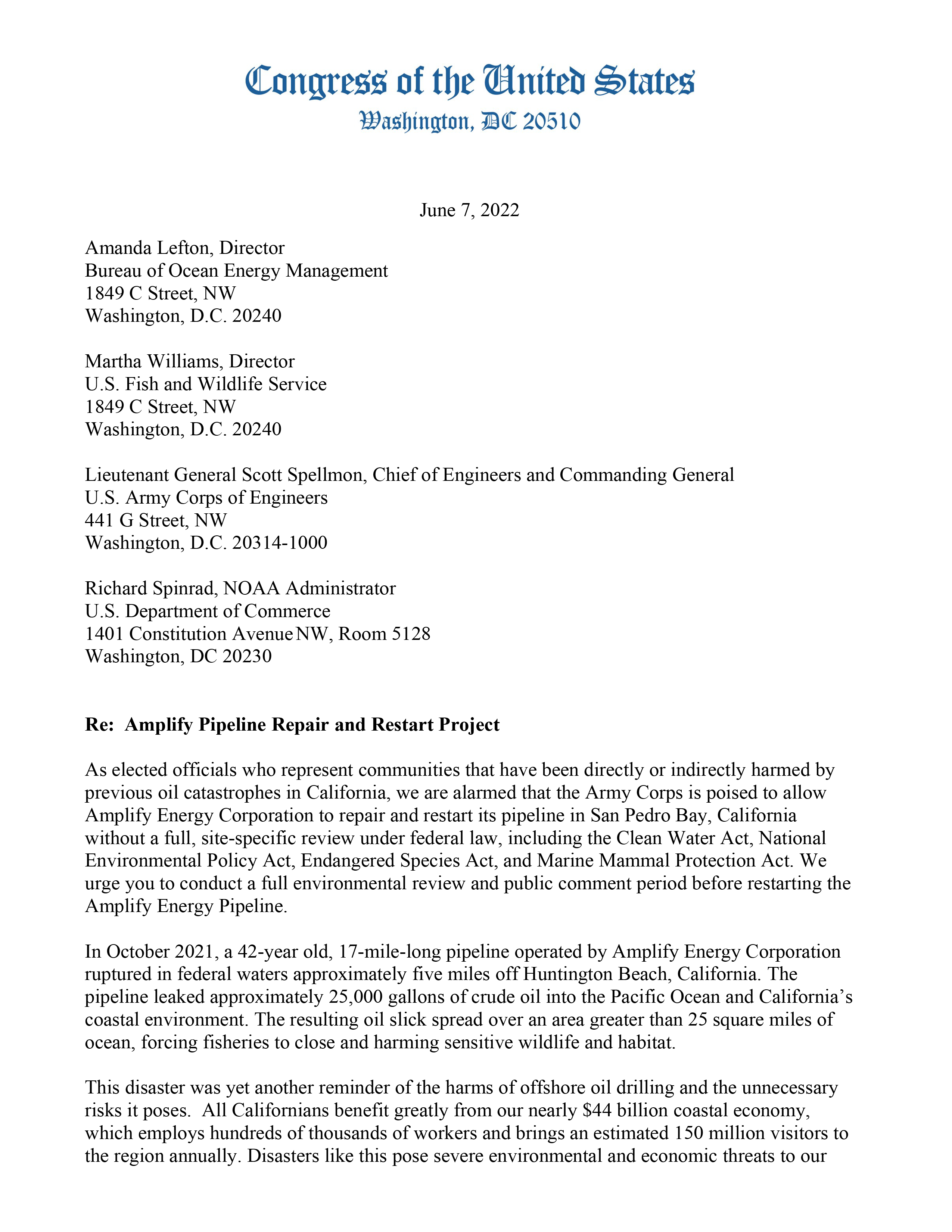
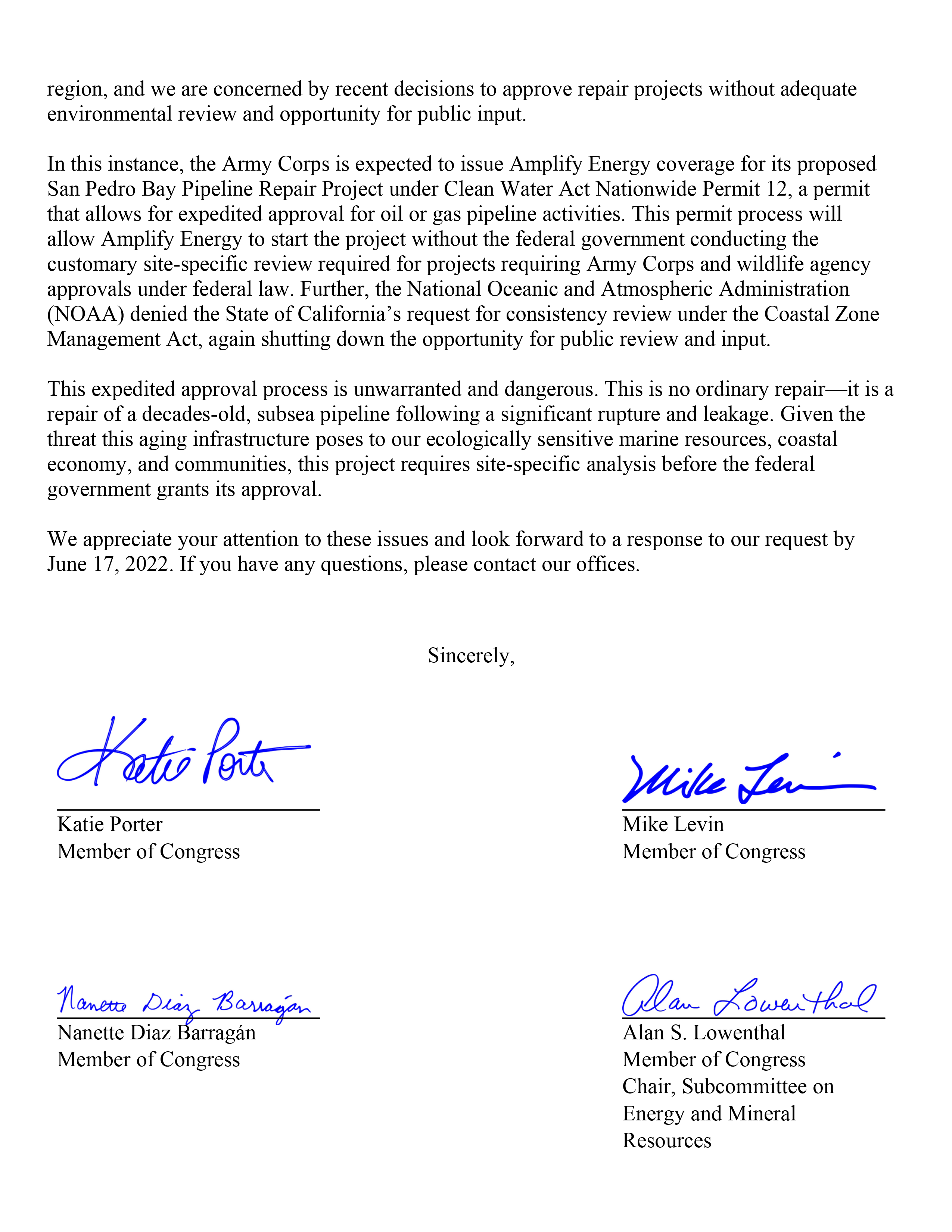
In terms of the total number of fatalities, the Piper Alpha fire was the worst disaster in the history of offshore oil and gas operations and sent shock waves around the world. Eight months later another interactive pipeline-platform fire killed 7 workers at the South Pass 60 “B” facility in the Gulf of Mexico. A US Minerals Management Service task group reviewed the investigation reports for both fires and recommended regulatory changes with regard to:
the identification and notification procedures for out-of-service safety devices and systems,
location and protection of pipeline risers,
diesel and helicopter fuel storage areas and tanks,
Lord Cullen’s comprehensive inquiry into the Piper Alpha tragedy challenged traditional thinking about regulation and how safety objectives could best be achieved, and was perhaps the most important report in the history of offshore oil and gas operations. Per Cullen:
“Many current safety regulations are unduly restrictive because they impose solutions rather than objectives. They also are out of date in relation to technological advances. Guidance notes lend themselves to interpretations that discourage alternatives.There is a danger that compliance takes precedence over wider safety considerations and that sound innovations are discouraged.“
Cullen advocated management systems that describe the safety objectives, the system by which those objectives were to be achieved, the performance standards to be met, and the means by which adherence to those standards was to be monitored. He called for safety cases that describe major hazards on an installation and provide appropriate safety measures. Per Cullen, each operator should be required in the safety case to demonstrate that the safety management systems of the company and the installation are adequate to assure that design and operation of the platform and its equipment are safe.
As we should and must, offshore operators, contractors, and regulators suffer over every injury, leak, or potentially hazardous event. This is also true for onshore oil and gas operations and most other industries. Yet for the past 2 years, we have been waiting for a proper investigation into the origins of the Covid virus. The Daily Mail is reporting that the Director-General of the WHO now believes that the virus was released from the Wuhan lab.
How can a company have a proper safety culture in a world where this level of malfeasance and stonewalling are tolerated and rewarded?
Kudos to BSEE’s Gulf of Mexico Region for their timely safety alerts and comprehensive updates on offshore incidents, trends, and compliance issues. Their most recent update is linked below.
For the past 50 years. my main goal for US offshore operations has been a zero fatality year. Sadly, that goal has never been achieved and will not be achieved this year (see slide 15).
Many casualties are associated with activities that are not perceived to be of high risk. The message on slide 22 of Jason’s presentation is thus very important:
Perceived low risk activities can still result in impactful injuries. Continually risk assess the work being undertaken, no matter if it permitted or nonpermitted work.
Know your personal limits and stop before you reach your limit. Pause and ask for help before you are at your limit.
“Our knowledge and expertise in geoscience and petroleum engineering represent advantageous foundation for CCS development, leading us towards our carbon emissions reduction target.”
Those who closely followed Australia’s Montara Inquiry in 2010 may be less convinced about PTTEP’s expertise. The Montara well suspension program was completely irresponsible. Even though the production casing cement was clearly compromised, PTTEP suspended the well without a single barrier in the well bore. The company was extremely lucky to have avoided a major safety, environmental, and economic disaster. Perhaps they are a very different company now; I certainly hope so.
Montara blowout, Timor Sea
The PTTEP announcement adds to our skepticism about the motives of some CCS proponents. Is CCS prudent public policy? That question is by no means settled and there has been very little opportunity for comment and debate. BOE has raised concerns and there are no doubt many more that have yet to be addressed.